INDICATIONS
Repatha® is indicated:
For US healthcare professionals
Repatha® is indicated:
For US healthcare professionals
Repatha® Plus a Statin Reduced the Risk of CV Events1,2
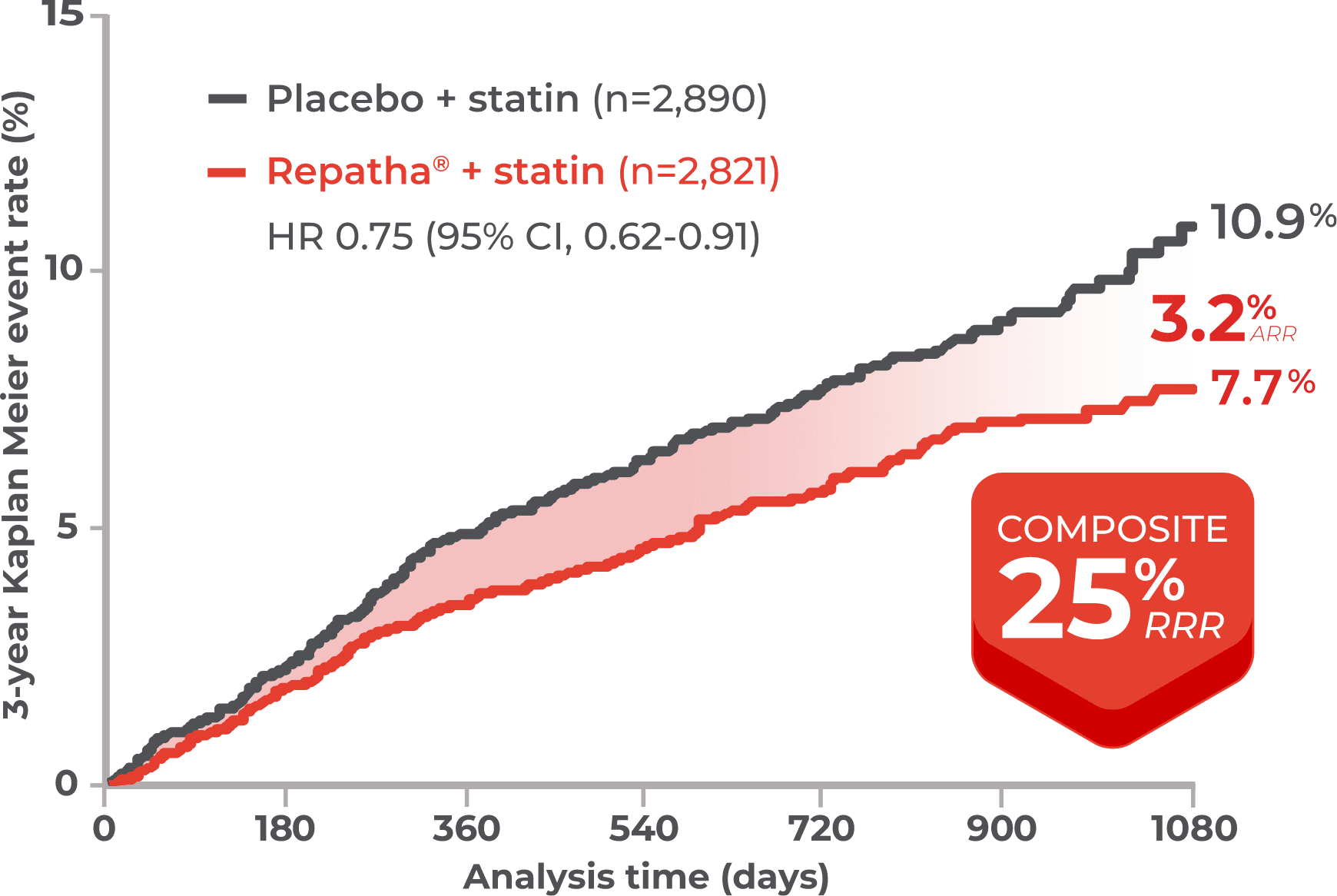
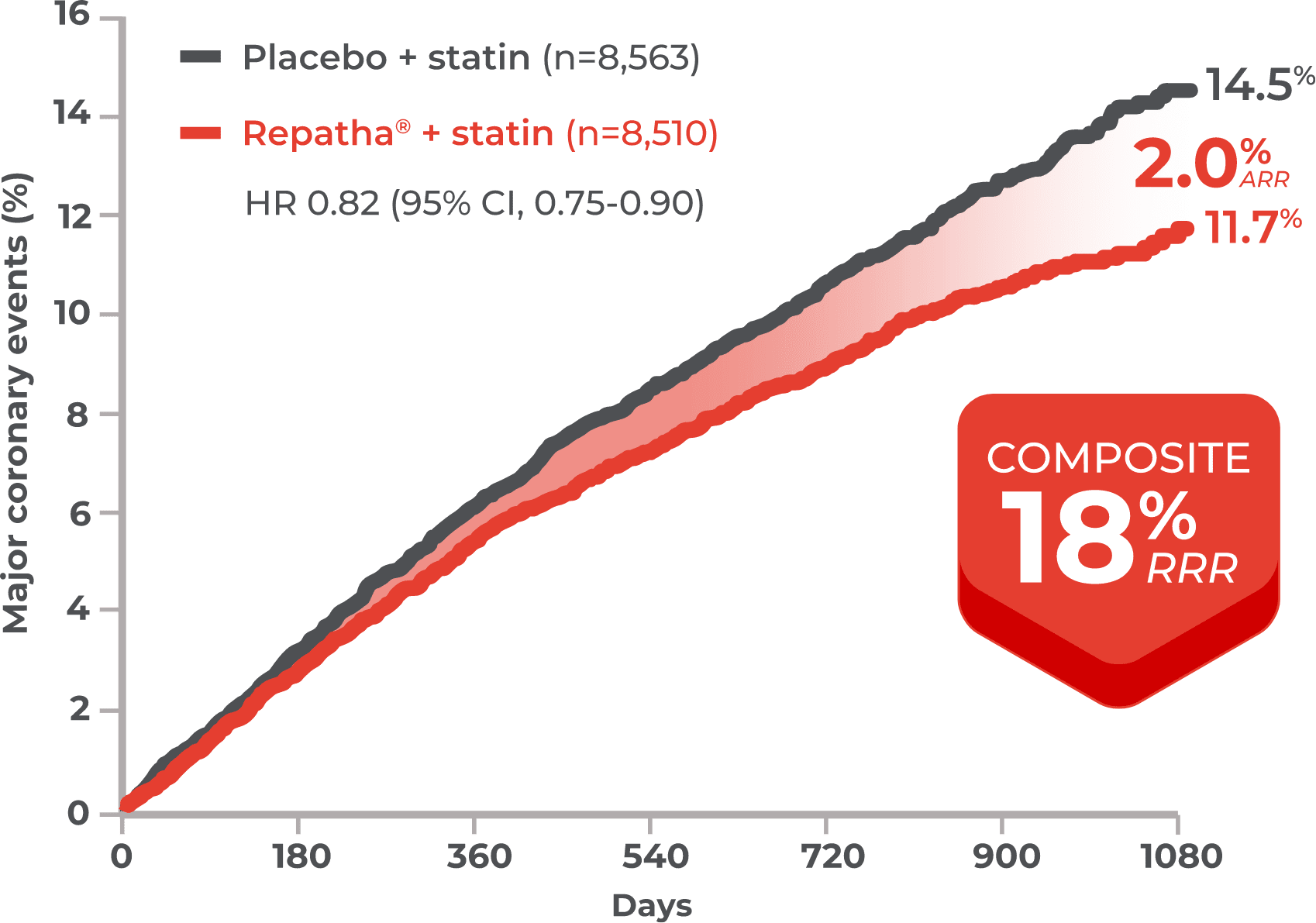
Repatha® + statin was proven to reduce the risk of composite CV events by 20% in a median of only 2.2 years, and the benefit improved over time in the study1,2
Key secondary endpoint: composite of time to first occurrence of CV death, MI, or stroke1,2

*Not statistically significant.
The FOURIER CV Outcomes Trial: A double-blind, randomized, placebo-controlled, event-driven trial of 27,564 patients with established CVD and LDL-C ≥70 mg/dL and/or non–HDL-C ≥100 mg/dL, despite high- or moderate-intensity statin therapy. Patients received either subcutaneous injections of Repatha® (evolocumab 140 mg every 2 weeks or 420 mg once monthly) or placebo. The median baseline LDL-C was 92 mg/dL.1,2



In a descriptive, retrospective analysis of 186,670 ASCVD patients with index LDL-C >70 mg/dL (mean index LDL-C of 108 mg/dL):
who intensified statins achieved LDL-C values ≤70 mg/dL12,*
who added ezetimibe to statin therapy achieved LDL-C values ≤70 mg/dL12,*
Patients were identified between January 1, 2012 and August 31, 2014, using the IQVIA US ambulatory electronic medical record database. Treatment exposure to statin and/or ezetimibe was based on observation of a valid prescription record in the EMR database, which does not guarantee that the patient filled the prescription or used the medication. This was a descriptive, retrospective analysis that evaluated the associations between exposures and outcomes but no causal relationships can be established from this observation study.12
*Baseline statin intensity: Among the 75,523 patients with ASCVD treated at baseline, 12.18% were on low statin intensity, 58.4% were on moderate statin intensity, 20.6% were on high statin intensity, and 8.8% were treated with other lipid-lowering agents.12
*Threshold for very high-risk ASCVD patients.
†The 2022 ACC Consensus Decision Pathway (referred herein as ACC Consensus Pathway) was designed to address current gaps in care for LDL-C lowering to reducing ASCVD risk. This effort relies extensively on the evidence established by the 2013 ACC/AHA and 2018 AHA/ACC/Multisociety cholesterol guidelines, and provides further recommendations regarding the use of newer nonstatin therapies. It should be noted that this process did not involve formal systematic reviews, grading of evidence, or synthesis of evidence. The goal was to provide practical guidance for situations not covered by the previously published guidelines until the next round of formal review of scientific evidence.13